Castleview clinic offers informative FAQs that cover a wide range of topics, including answers to the most popular questions our consultants get asked by our patients.
Frequently asked questions
What are the alternatives to knee replacement?
Most knee replacements are performed for osteoarthritis. Before surgery the mainstay of treatment for osteoarthritis of the knees is weight-loss and exercise.
Weight reduction can make a significant difference to symptoms and help should be sought with this as there are multiple services available via your GP and in the community. Gentle, regular exercise and muscle strengthening usually supervised by a physiotherapist, is also first-line treatment.
The National Institute of Clinical Excellence (NICE) recommends anti-inflammatory topical gels to apply directly to the knee, paracetamol and NSAIDs tablets (eg ibuprofen) for pain relief but we’d recommend asking your doctor about taking these medications long-term as they can have adverse effects especially on the stomach and kidneys.
When is the right age to have a knee replacement?
There isn’t a right age. Surgeons decide based on patients’ symptoms and how the pain and loss of function it is affecting your quality of life. The average age of a patient having a knee replacement in the UK is 70. In certain circumstances they are done in people in the 40’s and 50’s if the arthritis and daily symptoms are severe.
According to research and the National Joint Registry having a knee replacement when you are younger does carry with it a higher risk of dissatisfaction and a higher risk of revision (needing to have it done again).
Can I go running with a knee replacement?
Broadly the answer to this is no. Knee replacements are designed to allow sporting patients to go back to lower levels of sports (skiing, tennis, golf, racquet ball).
A short run, for example to the net for a drop shot in tennis will be possible but surgeons do not recommend training runs or jogging due to the risk that the knee replacement will come away from the bone (loosen) and need to be done again.
Can I play sport with a knee replacement?
Yes, but mostly at a low level only. Experienced athletes will be able to gently return to their sports except running. Our surgeons will take a history and advise you about your sports after a knee replacement and hopefully set your expectations at the right level.
At Castleview Clinic we have lots of testimonials of return to skiing, golf, cycling, hiking, tennis and other sports with the new knee.
Can I kneel with a knee replacement?
Knee replacements are not designed for kneeling however a lot of people can. After the surgery there is usually an area of numbness on the lateral side (outside) of the scar and then sensation of kneeling on this is often strange.
After the initial period of recovery from the surgery we recommend that you do try to kneel for gardening, housework etc. but always with a cushion or pad for protection of the knee.
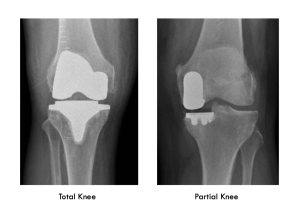
What is the difference between partial and total knee replacement?
Knee replacements are evolving all the time. The term knee replacement is actually fairly historic now as we mostly are only making very fine cuts to put new surfaces on the joint rather than replacing the knee bones.
The knee has three ‘compartments’: and outside and inside knuckle and an anterior compartment made by the knee cap joint. Total Knee Replacement resurfaces all three of these compartments in one go.
A ‘partial’ knee replacement is where the arthritis is mostly only affecting one of the three compartments and so only one compartment is resurfaced.
This can be done in up to 50% of cases and has the advantage of keeping most of your own knee with a quicker recovery from the surgery and a more normal feeling knee afterwards.
Further information on partial knees can be found at:
https://www.oxfordknee.com/oxford.html
How long do knee replacements last for?
The National Joint Registry (NJR) of the UK now has data for 18.5 years showing that upwards of 90% of total knee replacements are still in after this time.
The latest NJR report (2022) also shows that for the average patient having a new knee they will only need to have it done once in their lifetime. If the knee replacement is done in the earlier decades of life (40’s, 50’s and 60’s) the chances of it needing to be redone are higher.
https://reports.njrcentre.org.uk/Portals/0/PDFdownloads/NJR%2019th%20Annual%20Report%202022.pdf
Am I too young to have a knee replacement?
Surgeons make decisions about when to perform knee replacements based on multiple factors. We recommend surgery usually when the joint is completely worn out (grade 4 arthritis) on the Xray and your daily symptoms are severe.
The average age for a patient having a knee replacement in the UK is 70 but it may be appropriate to have one a lot younger than this depending on your own individual circumstances. Surgeons are cautious about perfoming knee replacements in younger patients for two main reasons. The first is studies show that dissatisfaction rates for knee replacements are higher in the younger age
groups.
Having the knee replacement in earlier in your life increases the possibility of the
replacement wearing out and it needing to be done again or even multiple times.
What are knee replacements made of?
Knee replacements are made of metal and plastic. The ends of the femur (thigh bone) and the top of the tibia (shin bone) are resurfaced with metal implants made of either titanium or an alloy of cobalt and chromium. These metal components are usually cemented on to the ends of the bone with bone cement (polymethylmethacrylate).
In orthopaedic surgery we do not use metal on metal bearings any longer so in between the two pieces of metal is fitted a piece of hard-wearing plastic called polyethylene. This plastic acts as the new ‘cartilage’ or bearing surface. In some instances the back of the kneecap is resurfaced in addition with another plastic bearing surface. The implants for each knee replacement, combined, weigh around 500 grams. (1 pound)
What are the alternatives to knee replacement?
Most knee replacements are performed for osteoarthritis. Before surgery the mainstay of treatment for osteoarthritis of the knees is weight-loss and exercise. Weight reduction can make a significant difference to symptoms and help should be sought with this as there are multiple services available via your GP and in the community. Gentle, regular exercise and muscle strengthening usually supervised by a physiotherapist, is also first-line treatment.
The National Institute of Clinical Excellence (NICE) recommends anti-inflammatory topical gels to apply directly to the knee, paracetamol and NSAIDs tablets (eg ibuprofen) for pain relief but we’d recommend asking your doctor about taking these medications long-term as they can have adverse effects especially on the stomach and kidneys.